
Contact



Address
Chair of Computer Science 5 (Pattern Recognition)
Martensstrasse 3
91058 Erlangen
Germany
Powered by

Dr.-Ing. Alexander Brost
Alumnus of the Pattern Recognition Lab of the Friedrich-Alexander-Universität Erlangen-Nürnberg
Combined Cardiac and Respiratory Motion Compensation for Atrial Fibrillation Ablation Procedures
 Alexander Brost, Wen Wu,
Alexander Brost, Wen Wu,  Martin Koch, Andreas Wimmer, Terrence Chen, Rui Liao, Joachim Hornegger, and Norbert Strobel
Martin Koch, Andreas Wimmer, Terrence Chen, Rui Liao, Joachim Hornegger, and Norbert Strobel
Atrial fibrillation (AFib) is widely recognized as a leading cause of stroke. An increasingly popular treatment option for AFib is catheter ablation during which the pulmonary veins attached to the left atrium (LA) are electrically isolated. These procedures are performed in electrophysiology (EP) labs often equipped with modern C-arm X-ray systems providing 3-D imaging of the heart [3]. The use of fluoroscopic overlay images, perspectively rendered from 3-D data sets,makes it possible to augment live 2-D X-ray projections with soft-tissue information. Unfortunately, catheter navigation using augmented fluoroscopy may be compromised by cardiac and respiratory motion. The first approach to overcome this problem, by providing a motion compensated fluoroscopic overlay image, has been proposed here. It involved tracking of a commonly used circumferential mapping (CFM) catheter firmly positioned at the ostium of the pulmonary vein in simultaneous biplane images. Drawbacks of this method are simultaneous biplane imaging and a need to detect when the CFM catheter has been moved from one PV to another. Another method for respiratory motion compensation has been introduced that tracks a catheter placed in the coronary sinus (CS) vein. Its drawback is that the CS catheter is far away from the site of ablation. As a consequence,it is not obvious that the motion derived from the CS catheter can be directly applied to compensation of both cardiac and respiratory motion. For example, relying on the CS catheter for motion compensation, we may encounter two problems. First, the correlation between the observed CS catheter motion and the actual motion required for dynamic overlay may be low. Second, the catheter in the coronary sinus may not always be visible due to collimation to reduce X-ray dose. Motion compensation using the CS catheter focused on 2-D motion compensation. Since simultaneous biplane fluoroscopy is hardly used in clinical practice, we also restrict ourselves to 2-D motion compensation as in previous approachs.
We present a novel method that combines the best ideas of the previous methods. The CS catheter is used as a point of reference to detect when the circumferential mapping catheter has been moved from one PV to another, while the motion estimate for adapting the fluoroscopic overlay is derived by localizing the CFM catheter. To obtain a good anchor point along the CS catheter, we decided to introduce a virtual electrode (VE). It is placed on the CS catheter more proximal than any other electrode.
Details can be found here.
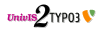
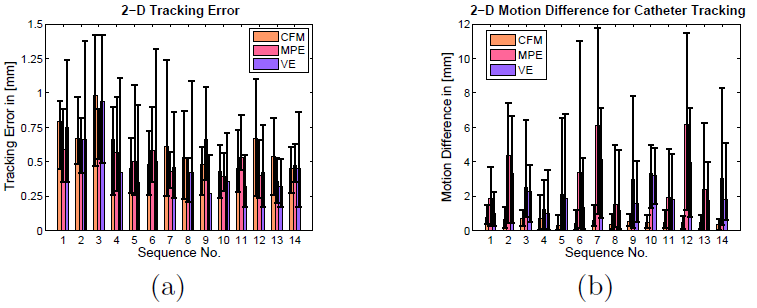
Our methods were evaluated on 14 clinical data sets from two different hospitals and from 10 different patients using leave-one-out validation. During three of these sequences, a 10-electrode CS catheter was used. In the remaining data sets, 4-electrode catheters were chosen. The images were either 512 × 512 pixels or 1024×1024 pixels. The pixel size varied between 0.173 mm and 0.345 mm. Image acquisition was performed without using ECG-triggered fluoroscopy. Hence, both respiratory and cardiac motion were present. At first, we evaluated the accuracy of the tracking methods. The localization error of the detected circumferential mapping catheter was calculated by considering the 2-D Euclidean distance to a gold-standard segmentation. To this end, the L2-distance transform of the gold-standard segmentation was calculated. The 2-D Euclidean distance was then obtained as the average over all values of the distance transform when evaluating it at the 2-D positions of the detected CFM. The gold-standard segmentation was manually generated for each frame in every sequence. The segmentation was supervised by an electrophysiologist. The localization accuracy of the coronary sinus catheter and the virtual electrode was calculated as the 2-D Euclidean distance to a gold-standard segmentation of the whole CS catheter. As before, the L2-distance transform was used. The results are given in Fig. 1(a). The CFM localization yielded an average 2-D error of 0.55 mm, which includes the inherent model error. The detection of the MPE on the CS catheter yielded an average 2-D error of 0.52 mm. The VE detection yielded an average 2-D error of 0.49 mm. Further, we compared the motion calculated from the catheter detection methods to the motion observed at the PV ostia. This motion was obtained by using a gold-standard segmentation of the circumferential mapping catheter. The center of the 2-D catheter model was used to calculate the underlying motion of the PV between successive frames. The comparison is given in Fig. 1(b). The motion obtained by CFM catheter detection differs on average by about 0.48 mm from the real motion, whereas the motion from the proximal CS electrode had a mean error of about 2.61 mm. Using the virtual electrode, we could reduce the mean error from 2.61 mm to 1.68 mm. The maximum difference between the true and the estimated motion using the CFM catheter was 2.06 mm. The MPE was off by up to 11.80 mm and the VE by up to 7.14 mm, see Fig. 1(b). The 14 fluoroscopic sequences used for evaluating the tracking performance had the CFM catheter firmly placed at a single pulmonary vein, i.e., the CFM catheter was not moved from one PV to the next. To evaluate our displacement detection method, five further sequences were added to our data set. To detect CFM catheter displacement, we introduced a displacement threshold. The displacement threshold is a percentage of the distance between VE and the center of the loop representing the CFM catheter. Results for different displacement thresholds are given in Tab. 1. The best result for displacement detection was found for an allowed change of the distance between 5 % and 10 %. A change in the absolute distance of 5 % turned out to be the best threshold for detecting catheter repositioning in our experiments. In this case, the false positive rate was 5.8 %. We decided on the VE for displacement detection, because it turned out to be a much more stable reference than the MPE. This can be seen, e.g., by taking a look at their mean errors and maximum differences, see Fig. 1(b).
 |
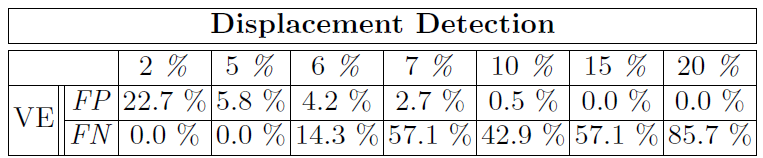 |
The results indicate that our catheter localization and tracking algorithms are accurate enough to meet clinical needs, cf. Fig. 1(a). In our experiments, involving non-ECG-triggered X-ray data acquired under free breathing conditions, only tracking of the CFM was accurate enough to be directly applicable to motion compensation without any need for a more sophisticated motion model, see Fig. 1(b). The tracking of the circumferential mapping catheter yielded an overall average error of 0.55 mm. Since this error also contains some model error of the underlying B-spline catheter model, which is not adapted over time, the actual tracking performance of the distance-transform-based method is even better. The motion difference between the real motion at the PV ostia and the estimated motion, yielded a maximum error of 2.06 mm. The same error for the MPE was 11.80 mm and 7.14 mm for the VE, respectively, see Fig. 1(b). From these numbers, we conclude that the circumferential mapping catheter is the best surrogate for the motion of the left atrium. A visual comparison between motion compensation using the CFM and the VE is given in Fig. 2. At first sight, our observations seem to contradict the results reported with different approaches. Maybe the varying results are due to differences in how the procedures were performed. For example, some centers apply general anesthesia while only mild sedation was used in our cases. Some clinical sites also provide a setup where ECG signals can be recorded on the fluoroscopy system. The ECG could be exploited to select proper fluoroscopic frames. As our cases came from multiple sites using different ECG recording equipment, we decided to not take advantage of any ECG signals to keep things consistent. The choice for one method or the other may come down to how well you control the procedure. For example, if there is general anesthesia, stable sinus rhythm, and available ECG information, the approach presented in literature may be the method of choice. However, in the general case it may not be straightforward to apply it as successfully. Although we found it difficult to rely on the CS catheter for motion compensation, we observed that it could be used to detect displacement of the CFM catheter. If the distance between the circumferential mapping catheter and the virtual electrode changes by a certain amount, we assume that the mapping catheter has been moved from one PV to the other. From our experiments, using the absolute distance between the CFM and the VE yielded the best results to detect that the CFM moved away from a particular PV. A change in the absolute distance of 5 % was the best threshold in our experiments yielding a false positive rate of 5.8 %. Compared to a misdetection which may lead to incorrect fluoroscopic overlays, a false detection is preferred. At most, there are a few frames without motion correction.
 |
Full paper available here.
